FOIA Obstruction, Records Access Failure, Administrative Exhaustion, Evidence Erasure, ADA Process Barrier, ADA Catch-22, Whistleblower Records Obstruction, Medicaid Records Access, Public Records Civil Rights, Search Certification, Evidence Preservation Failure, Administrative Weaponization, Disability Rights Obstruction, FOIA Accountability, Civil Rights Process Failure, Medicaid Whistleblower Protection, Hidden Records Civil Rights, Process as Retaliation, Public Records Transparency, Administrative Accountability, Constitutional Rights, Section 504 Access, Olmstead Records, Provider Choice Proof, Federal Oversight Failure
When Records Are Hidden, Rights Become Unreviewable The Weaponization of FOIA, ADA Process, and Administrative Exhaustion Against Medicaid Whistleblowers How public records obstruction, inaccessible complaint systems, and evidence erasure can protect closed Medicaid systems from review

When Records Are Hidden, Rights Become Unreviewable
The Weaponization of FOIA, ADA Process, and Administrative Exhaustion Against Medicaid Whistleblowers
How public records obstruction, inaccessible complaint systems, and evidence erasure can protect closed Medicaid systems from review
Civil rights do not only fail in court.
They fail when the records needed to prove a violation are hidden.
They fail when public agencies delay, fragment, or deny access to the documents that show how decisions were made.
They fail when a person with a brain injury is forced to navigate complex complaint systems without reasonable communication support.
They fail when the administrative process becomes so confusing, hostile, and exhausting that the person reporting the violation becomes the one blamed for not surviving the process.
That is the next national issue identified through the David Medeiros record.
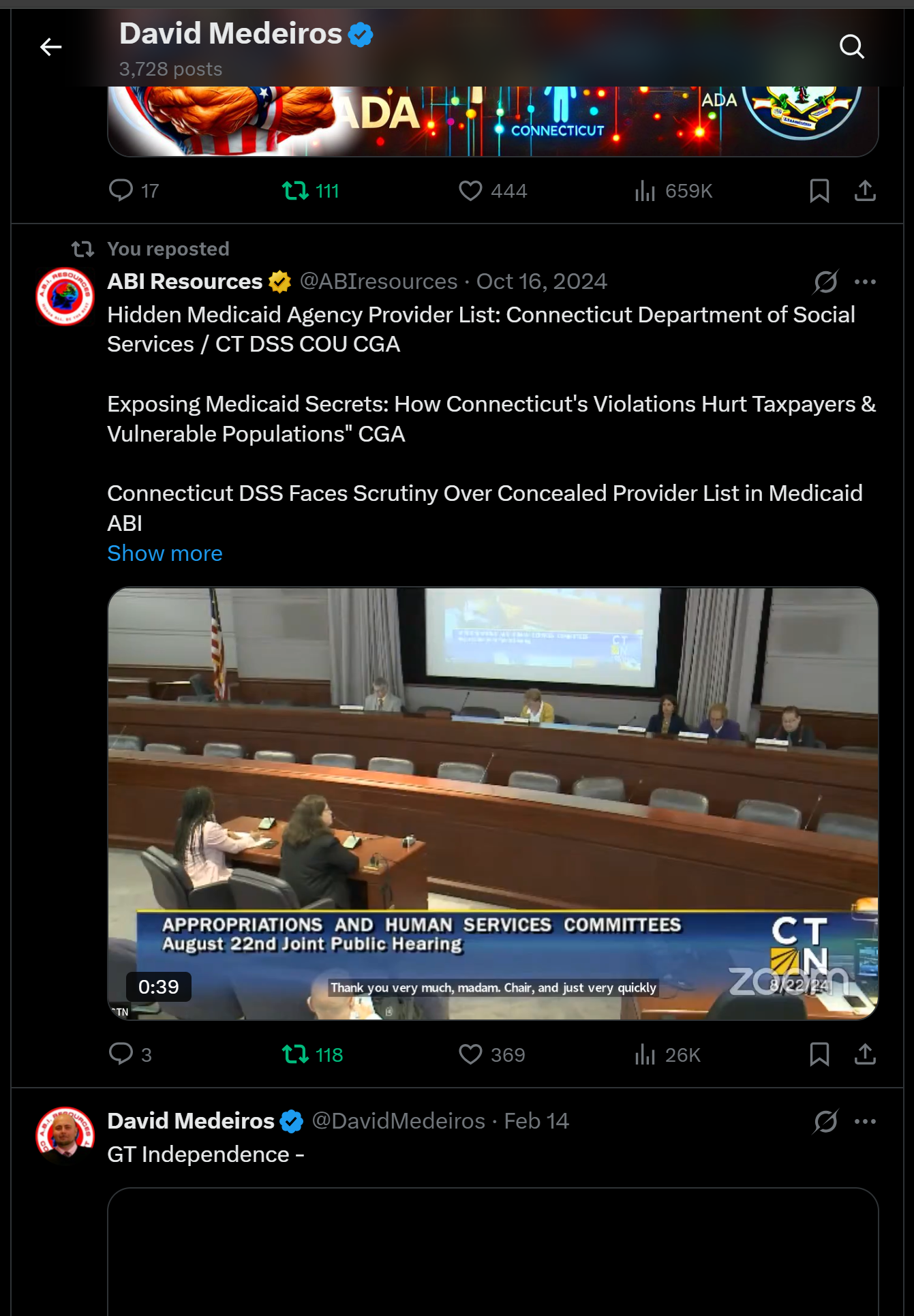
David Medeiros of Connecticut is a brain injury survivor, stroke survivor, founder of ABI Resources, Medicaid Acquired Brain Injury Waiver provider, disability rights advocate, and public whistleblower. His record connects Medicaid provider choice, ADA communication access, Section 504, Olmstead community integration, FOIA evidence access, DOJ Civil Rights reports, CHRO process concerns, DSS Medicaid administration, CMS oversight, HHS OCR enforcement, HHS OIG program integrity, whistleblower retaliation, federal coordination, public records obstruction, third party transparency platform disruption, and evidence preservation.
The prior articles asked whether disabled Medicaid families were shown real provider options.
This article asks a deeper question:
What happens when the records that prove provider choice, ADA access, Medicaid compliance, and retaliation are delayed, denied, deleted, fragmented, or made inaccessible?
The answer is direct:
When records are hidden, rights become unreviewable.
Why this article comes next
This article comes next because it closes the proof loop.
The Provider Choice Receipt shows what families should receive.
The federal provider verification website shows how families should confirm provider options.
The Accountability Dashboard shows how agencies should measure performance.
The First 100 Days plan shows how agencies should preserve, classify, route, and correct complex disability rights matters.
Now this article explains the obstruction layer.
The obstruction layer is where agencies prevent the truth from becoming reviewable.
That can happen through:
Delayed records responses.
Incomplete searches.
No records claims without search certification.
Overbroad privacy claims.
Fragmented email threads.
Inaccessible complaint systems.
Ignored ADA accommodation requests.
Deleted or missing evidence.
Closed cases without meaningful review.
Third party transparency records becoming unavailable.
Repeated agency referrals that leave no accountable owner.
Exhaustion of the whistleblower through procedural burden.
This is why the article matters.
If provider choice was denied, records prove it.
If ADA accommodations were ignored, records prove it.
If retaliation followed protected reporting, records prove it.
If Medicaid funds moved through a closed referral system, records prove it.
If records are hidden, every one of those rights becomes harder to enforce.
The constitutional democracy principle
Public records are not paperwork.
They are the civic audit trail.
They show who knew what.
They show when agencies were notified.
They show whether deadlines were followed.
They show whether provider lists existed.
They show whether families received those lists.
They show whether Medicaid choice was real.
They show whether accommodations were requested.
They show whether accommodations were denied.
They show whether complaints were routed.
They show whether cases were closed without review.
They show whether evidence was preserved.
They show whether public money followed lawful service delivery.
In a functioning system, records allow the public to compare what an agency says with what the agency did.
That is why records access is not a side issue.
It is the foundation of civil rights review.
The legal foundation
Federal FOIA requires federal agencies to determine within twenty working days whether to comply with a records request, excluding Saturdays, Sundays, and legal public holidays, and to notify the requester of the determination, reasons, appeal rights, and access to FOIA assistance.
ADA Title II requires state and local governments to give people with disabilities equal opportunity to benefit from public programs, services, and activities. DOJ states that Title II applies to state and local programs such as health care, social services, courts, voting, emergency services, and government offices.
DOJ effective communication guidance states that covered entities must communicate effectively with people with communication disabilities and must consider the nature, length, complexity, and context of the communication and the person’s normal communication method.
Section 504 prohibits disability discrimination in programs and activities receiving federal financial assistance. HHS OCR states that Section 504 applies to federally funded health and human service programs, including health care providers participating in Medicaid and CHIP, state and local human service agencies, and nursing homes.
Federal Medicaid freedom of choice rules state that a beneficiary may obtain Medicaid services from any qualified provider willing to furnish those services, subject to lawful exceptions.
CMS states that the Medicaid Access Final Rule advances access and quality across Medicaid, including HCBS, and strengthens oversight of person centered planning, incident management, grievance systems, waiting list reporting, service delivery timeliness, HCBS quality measures, and public transparency.
These laws and policies all point to one conclusion:
A disabled person must be able to access the process, access the records, understand the communication, preserve the evidence, and obtain review.
The central thesis
The central thesis of this article is:
Administrative obstruction can become civil rights obstruction when agencies use records delays, inaccessible processes, fragmented communication, and evidence loss to make disability rights violations impossible to prove.
This is not only about one request.
This is not only about one agency.
This is not only about one closed case.
The bigger issue is whether public agencies can use procedure to prevent review.
When the answer is yes, administrative process becomes a shield.
When the person affected has a brain injury, inaccessible process becomes a disability rights issue.
When Medicaid funding is involved, records obstruction becomes a federal accountability issue.
When provider choice is at stake, hidden records can affect the lives of disabled people and families.
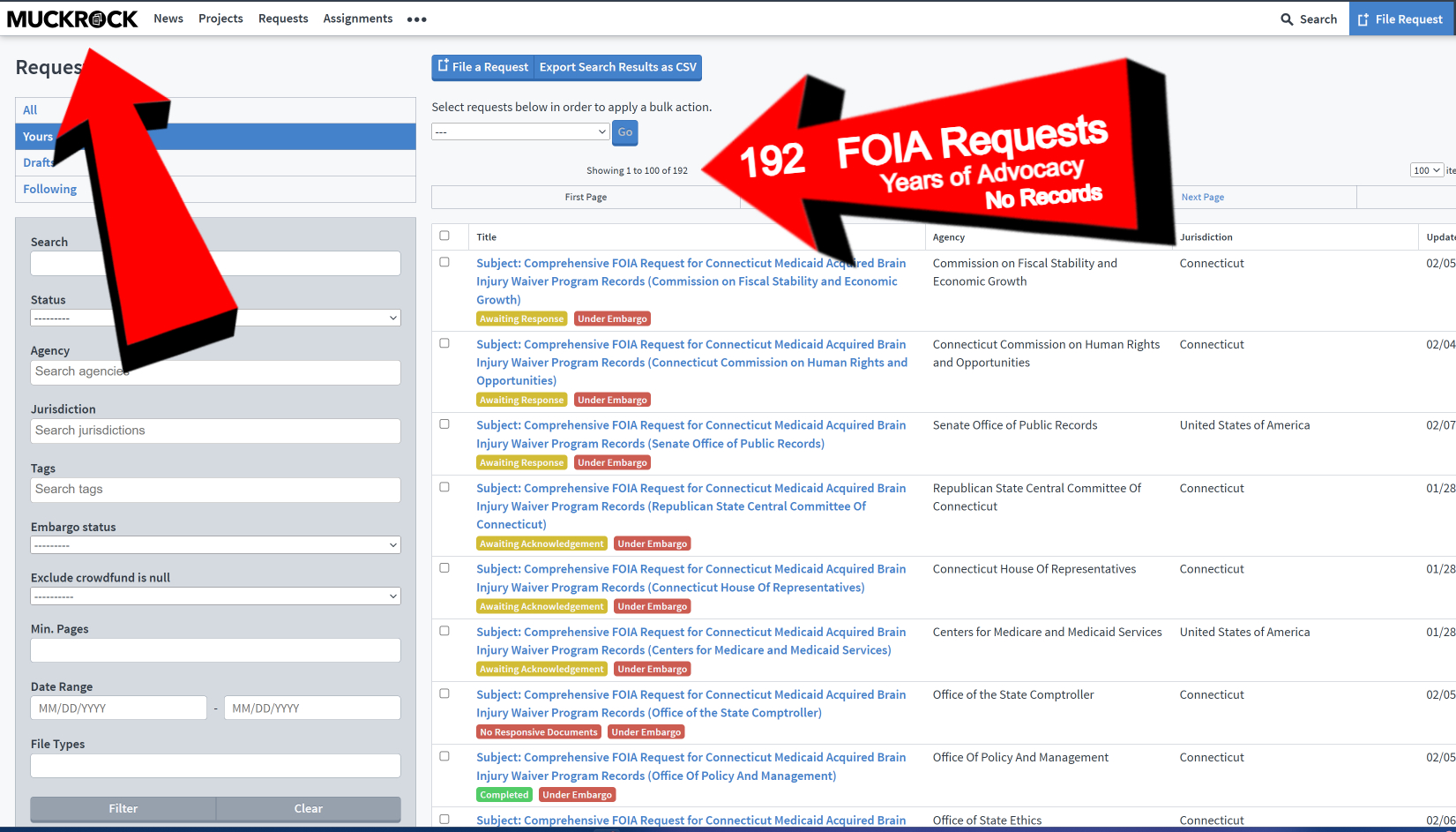
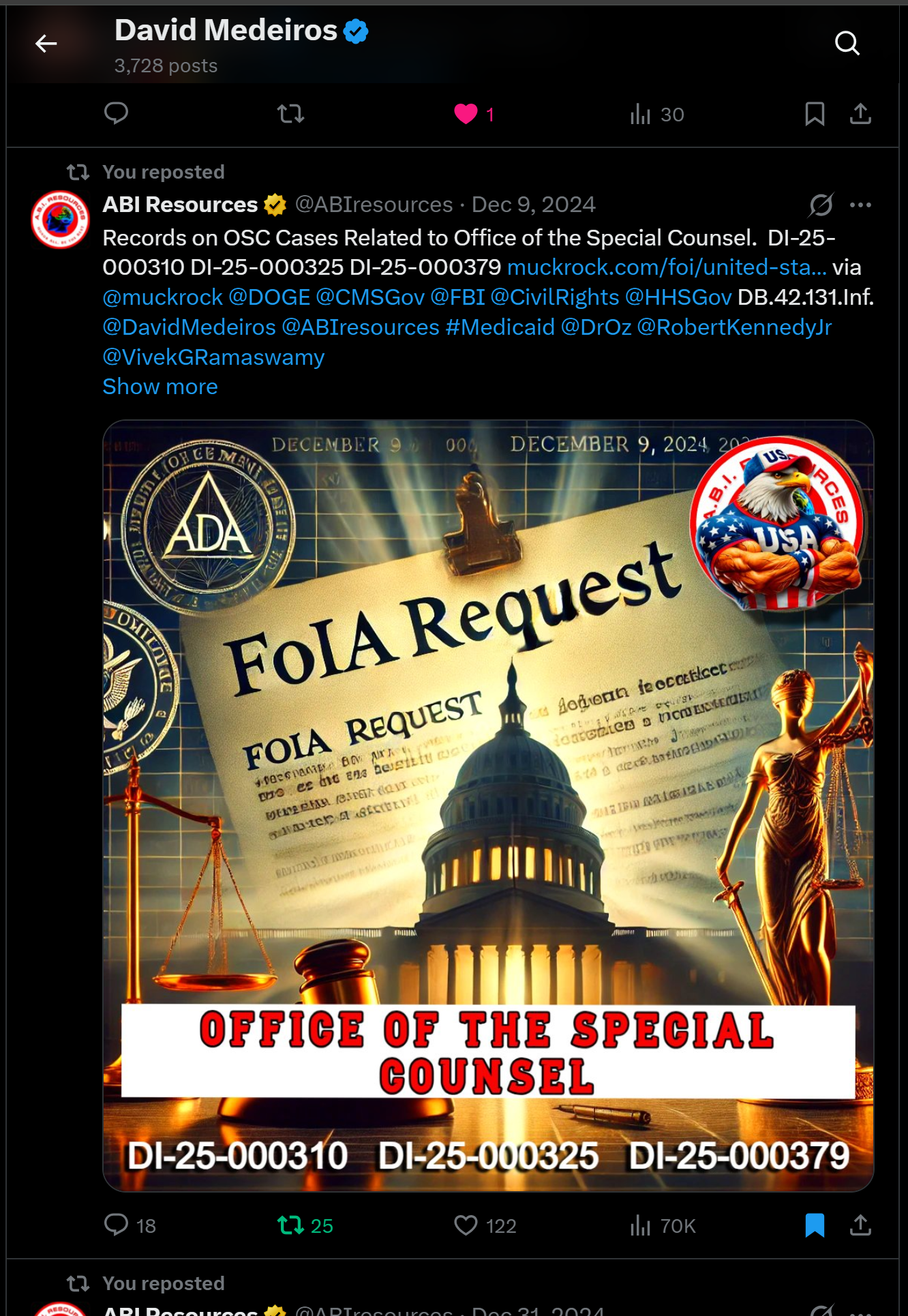
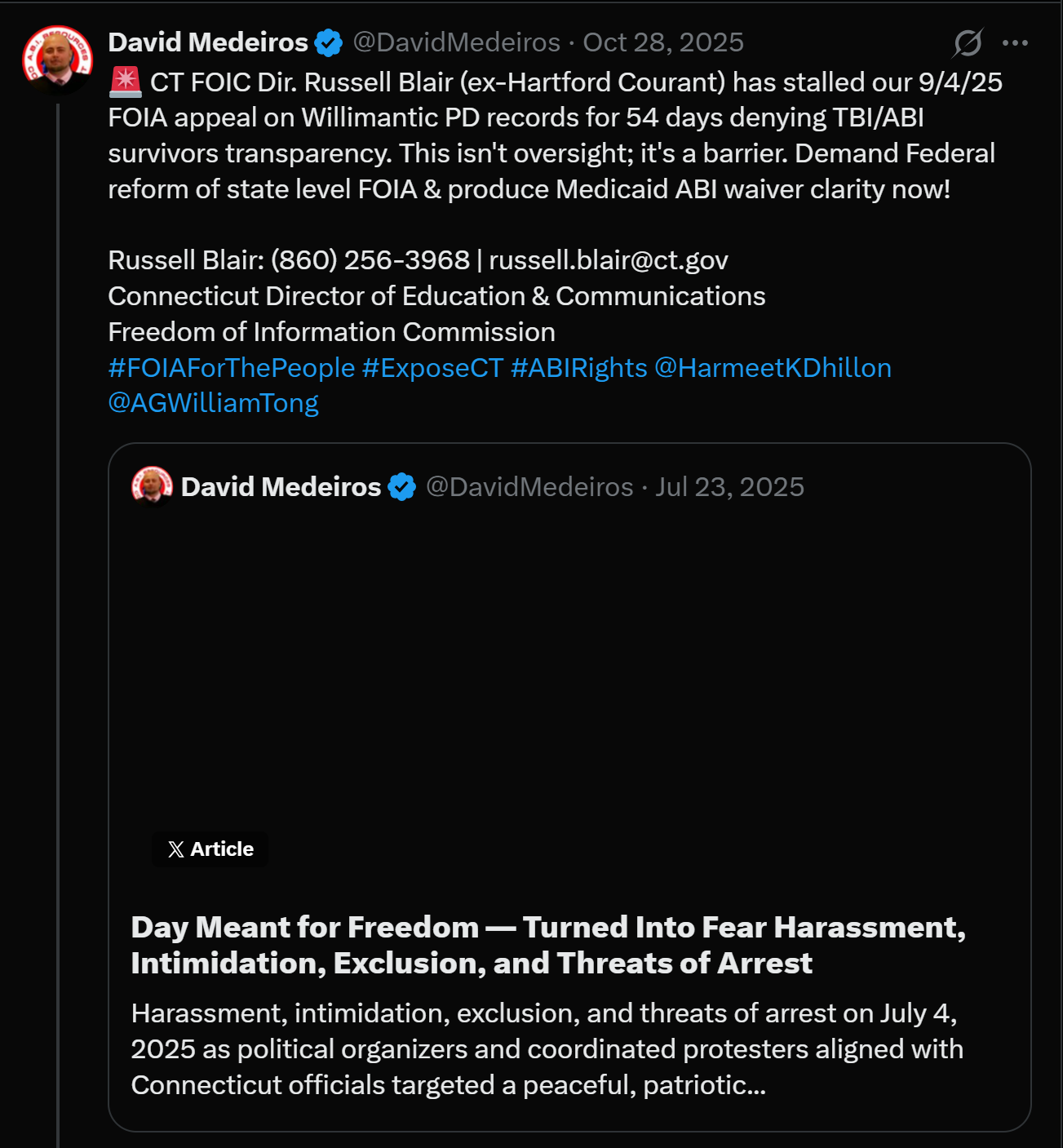
The FOIA blockade
To prove a Medicaid provider choice problem, the first question is simple:
Where is the full provider directory?
For the Medicaid ABI Waiver system, that question matters because provider choice cannot be meaningful if families are not shown every qualified willing provider.
Federal Medicaid rules protect the ability of beneficiaries to receive services from qualified willing providers, subject to lawful exceptions.
But the right becomes weak when families cannot see the provider options.
The right becomes weaker when advocates cannot obtain the provider directory.
The right becomes weaker still when public records requests are delayed, denied, fragmented, or answered without search detail.
A real records response should answer:
What provider directory existed?
Who maintained it?
What dates did it cover?
What providers were listed?
Which providers were active?
Which providers served which regions?
Which providers accepted referrals?
Which families received the directory?
Which care managers used it?
Which records show provider selection?
Which records show referrals?
Which records show service authorization?
Which records show Medicaid payment?
Without those records, oversight becomes guesswork.
The difference between privacy and accountability
Privacy laws protect people.
They should not be misused to hide public system operations.
Patient health information deserves strong protection.
Private medical records should not be exposed.
Participant identities should not be published without lawful authority.
But provider directories, public contracts, provider enrollment records, agency procedures, aggregate referral data, deidentified utilization data, policy communications, and system level audit trails are not the same as private medical records.
A lawful system can protect patient privacy while still releasing public accountability records.
The proper question is not:
Can the agency hide everything because Medicaid involves health care?
The proper question is:
What can be released, redacted, deidentified, or certified so the public can verify whether the program followed the law?
Privacy should not become a blanket for secrecy.
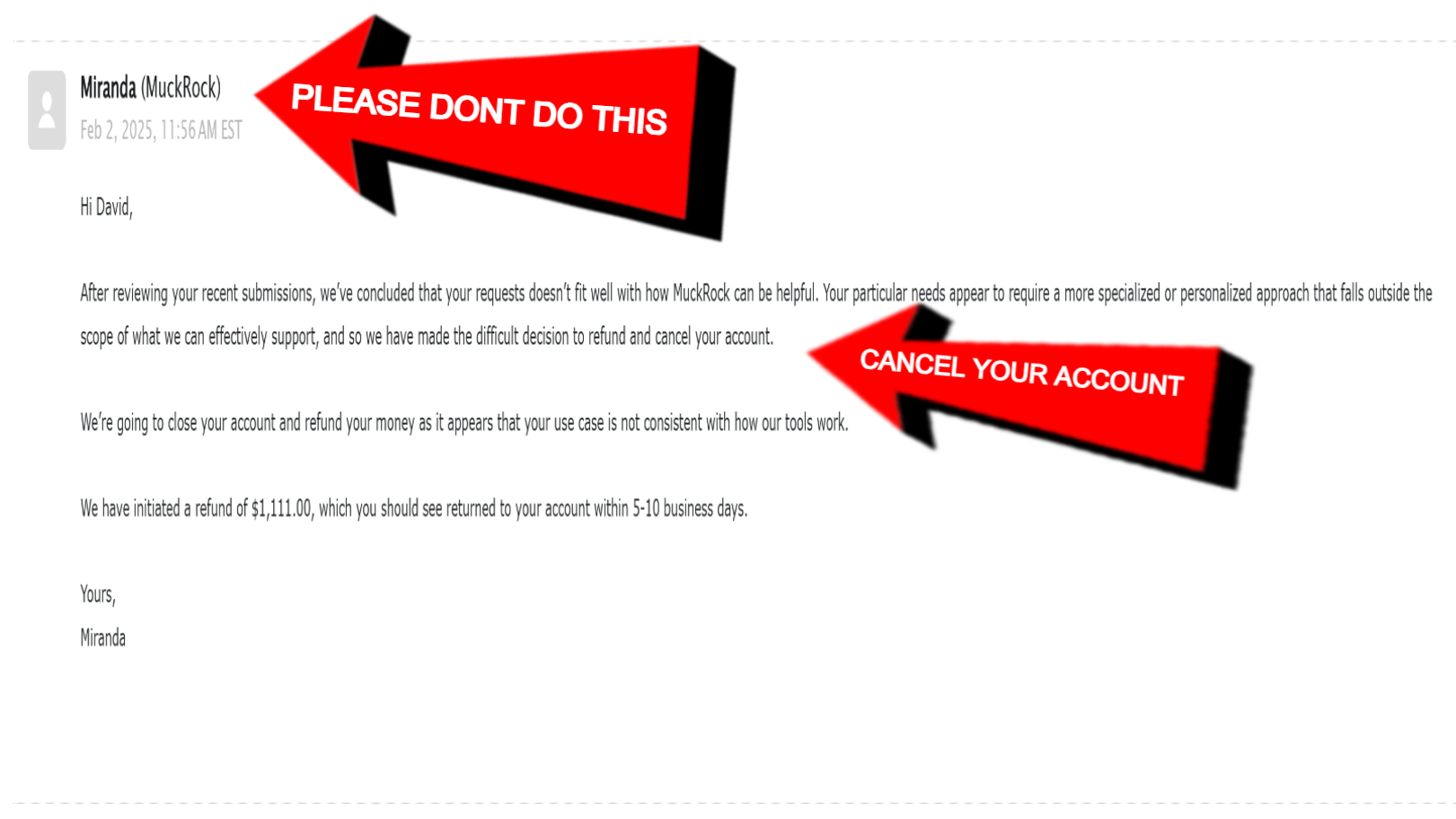
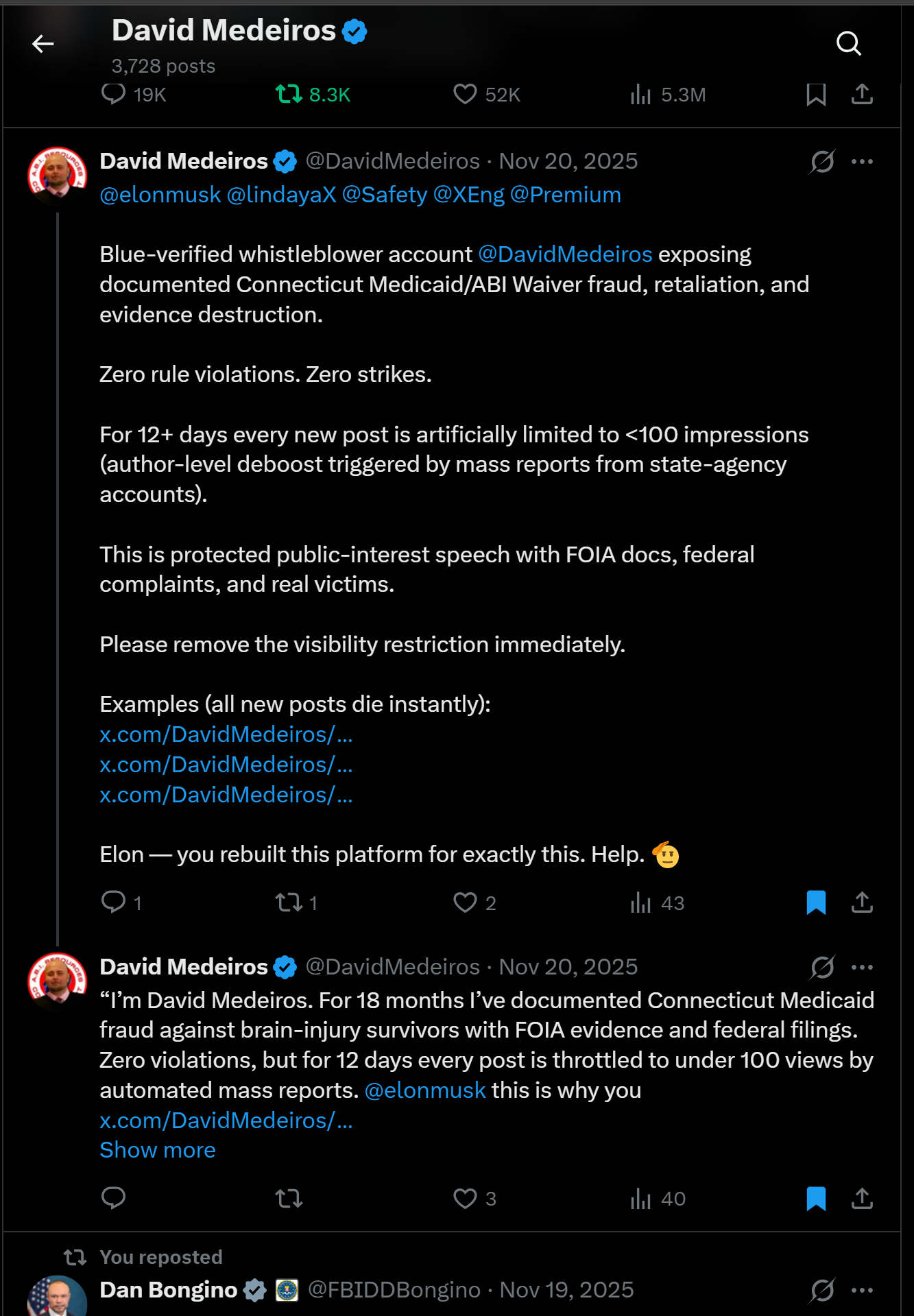
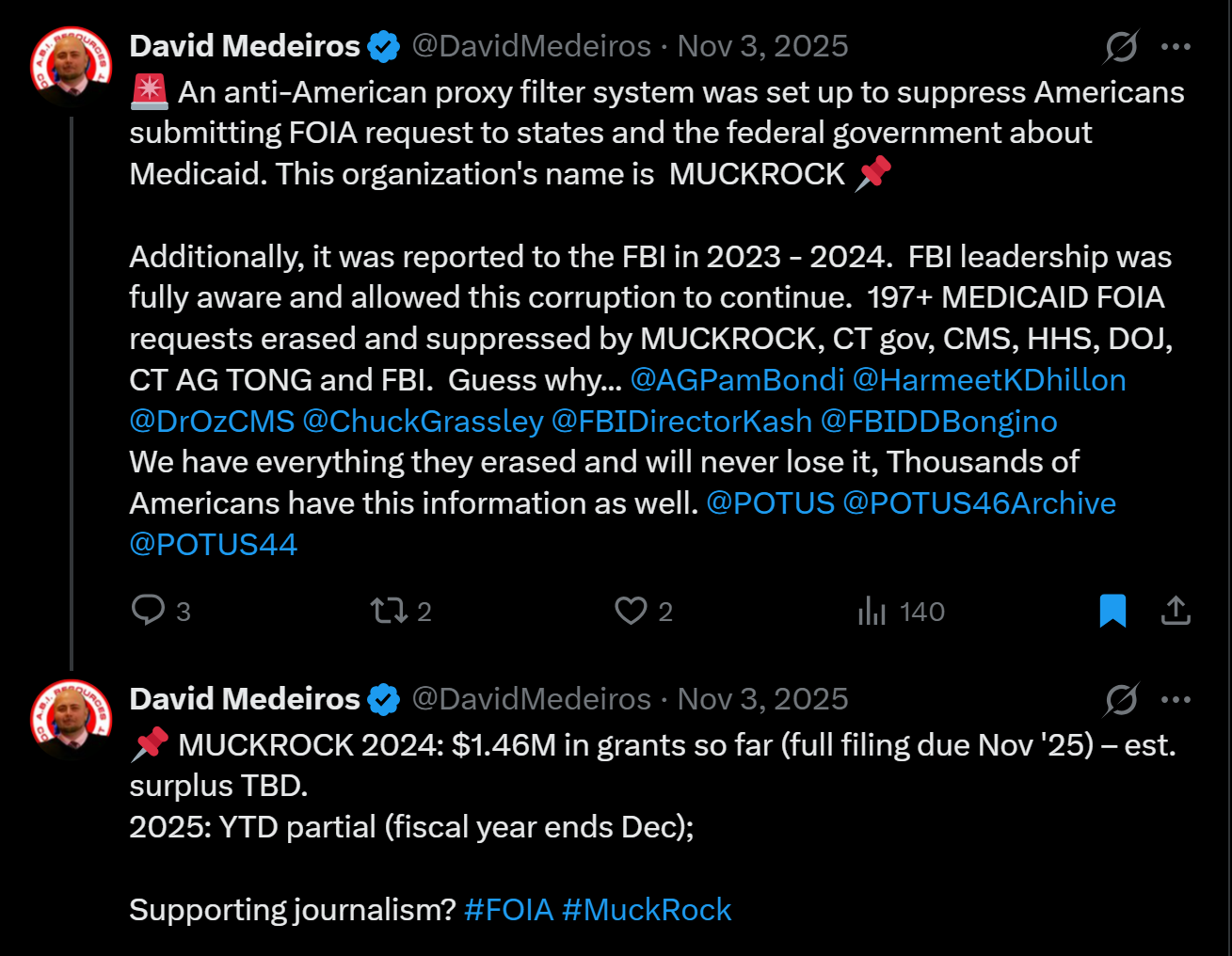
The MuckRock issue
The source text provided for this article identifies MuckRock account termination and FOIA digest disruption as a key evidence issue. It frames the concern as a third party transparency platform disruption connected to the public records trail.
This issue should be framed carefully.
The public question is not whether every technical event has already been proven as intentional destruction.
The public question is whether the public records trail remained intact, accessible, preserved, and independently verifiable.
When a third party transparency record becomes unavailable, investigators should ask:
What requests were filed?
What agencies received them?
What responses were issued?
What records were published?
What records disappeared?
What account access changed?
What notices were sent?
What backups exist?
What metadata exists?
What communications occurred between agencies and the platform, if any?
What logs can verify what happened?
Were any public records tracking links broken?
Were any records removed from public view?
Were any account actions triggered by complaints, legal requests, moderation, user action, platform policy, or technical failure?
That is the correct oversight frame.
The issue is evidence preservation.
The issue is public traceability.
The issue is whether the records trail survived.
The ADA Catch 22
The ADA Catch 22 is the most important disability rights concept in this article.
It happens when a disabled person must use an inaccessible process to report that the process is inaccessible.
For a brain injury survivor, this can include:
Too many email threads.
Too many portals.
Dense legal language.
Unclear deadlines.
Unclear case numbers.
No single point of contact.
No written summary.
No plain language explanation.
No accommodation decision in writing.
Repeated requests to resubmit the same information.
Fragmented agency referrals.
Procedural penalties for cognitive fatigue or memory limitations.
This is not just bad customer service.
In a government process covered by ADA Title II or Section 504, it can become a civil rights access issue.
DOJ says state and local governments must give people with disabilities equal opportunity to benefit from public programs, services, and activities.
DOJ also states that effective communication depends on the nature, length, complexity, and context of the communication.
A Medicaid whistleblower record involving FOIA, ADA, Section 504, provider choice, CHRO, DSS, DOJ, HHS OCR, CMS, HHS OIG, Medicaid funding, and retaliation is complex by nature.
That complexity triggers a higher need for accessible communication.
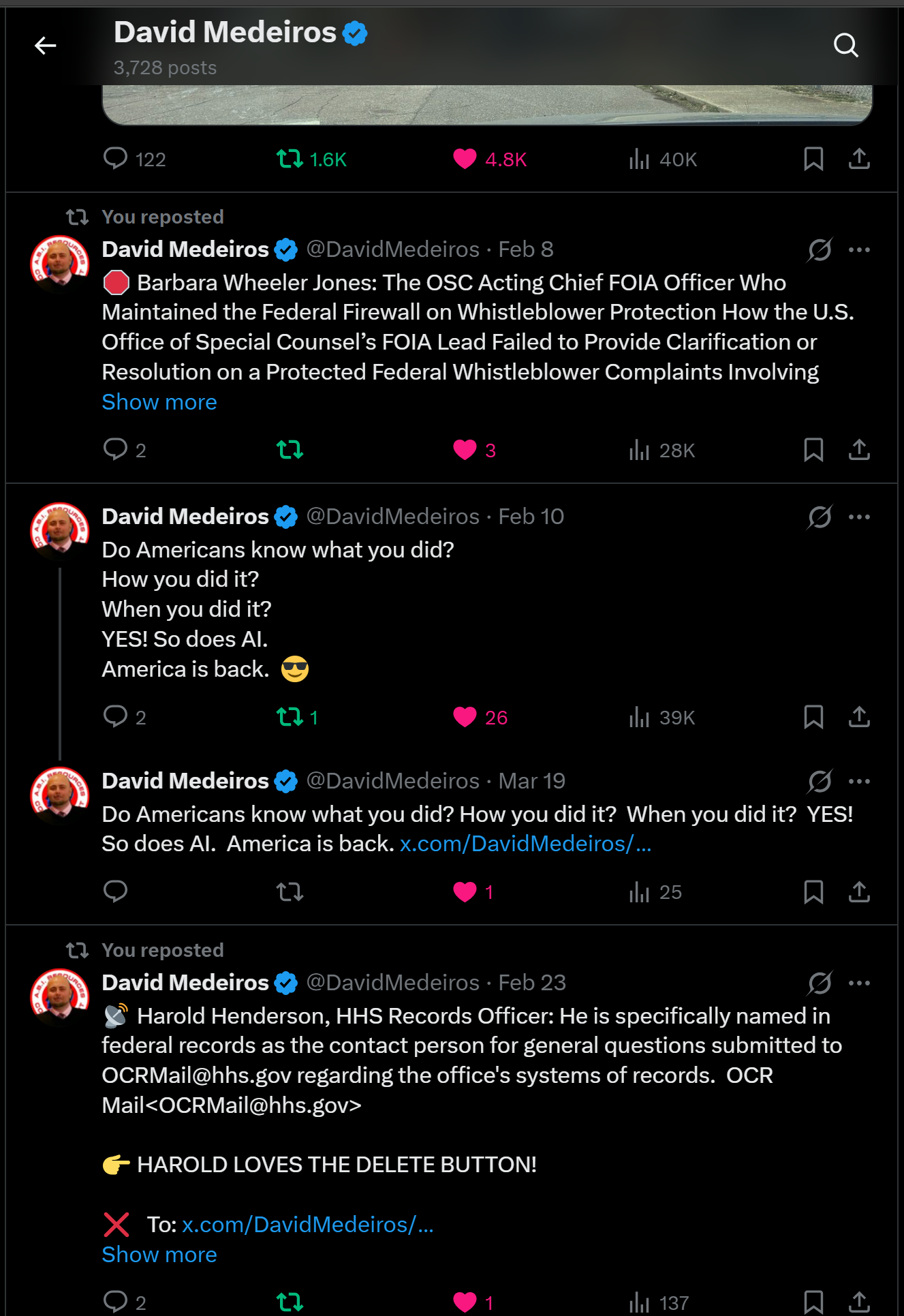
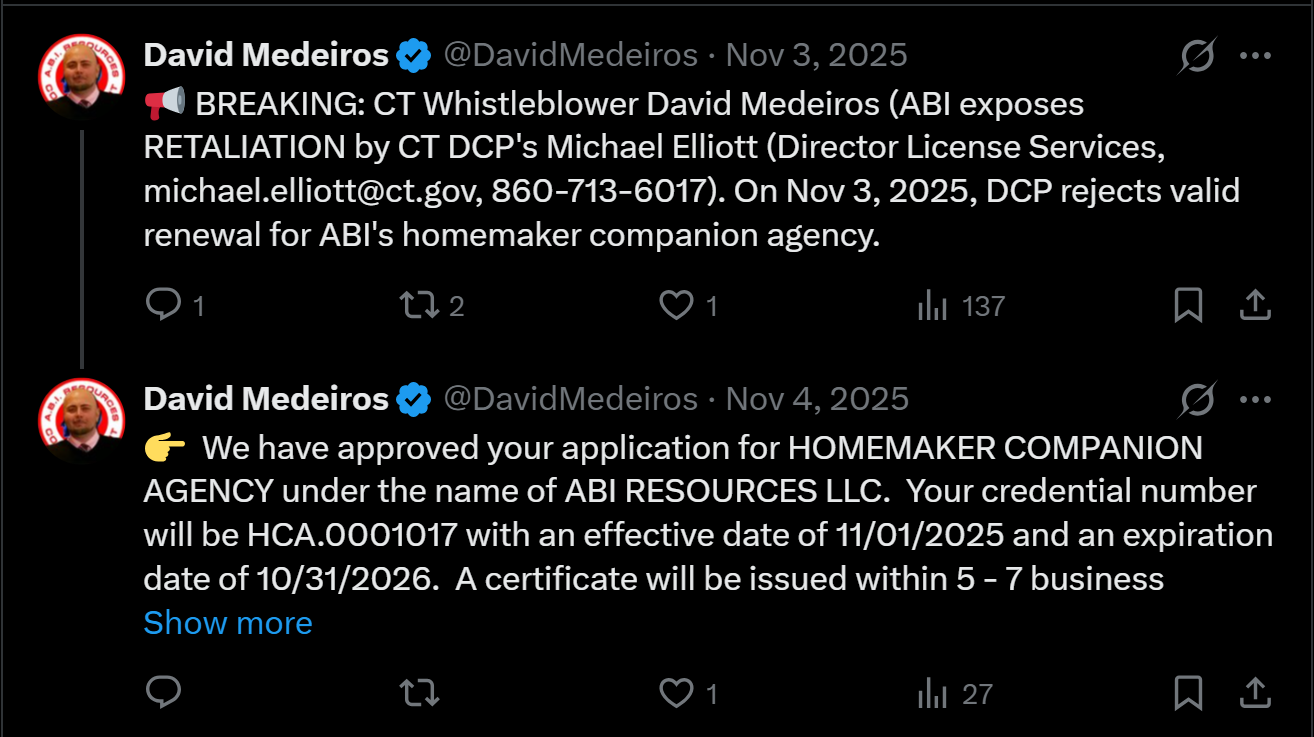
How process becomes retaliation
Retaliation is not always loud.
It can be procedural.
It can look like delay.
It can look like silence.
It can look like a missing record.
It can look like a refusal to consolidate communication.
It can look like repeated referrals.
It can look like a portal that accepts evidence but produces no meaningful review.
It can look like a closure letter that does not address the core evidence.
It can look like a records search that never identifies who searched, what systems were searched, or what terms were used.
It can look like a disabled person being forced to repeat the same facts until exhaustion becomes inevitable.
For a whistleblower, administrative burden can become a pressure system.
For a person with a brain injury, administrative burden can become an access barrier.
For Medicaid families, administrative burden can keep provider choice hidden.
For agencies, administrative burden can become a way to avoid accountability without issuing a direct denial.
That is why process must be measured.
The inaccessible intake problem
Civil rights intake systems often count reports.
They issue confirmation numbers.
They send automated emails.
They close reports.
But the key questions are different:
Did the system understand the disability access issue?
Did it identify Medicaid funding?
Did it identify Section 504?
Did it identify ADA Title II?
Did it identify provider choice?
Did it identify Olmstead risk?
Did it identify retaliation?
Did it identify records obstruction?
Did it identify evidence preservation needs?
Did it refer the matter to the correct agency?
Did it preserve attachments and metadata?
Did it provide accessible status updates?
Did it explain why no further action was taken?
Did it connect repeated related reports?
An intake system that receives reports but does not connect patterns may protect the appearance of review while failing the substance of review.
Why FOIA and ADA are connected
FOIA and ADA are often treated as separate issues.
They are not separate when the requester is disabled and the records are needed to prove a disability rights violation.
For a person with a brain injury, records access may require:
Written communication.
Clear step by step instructions.
Plain language summaries.
Stable tracking numbers.
One point of contact.
Extra time.
Accessible electronic files.
Search explanations.
Status updates.
Consolidated communications.
If an agency provides records access only through a confusing, fragmented, inaccessible process, the records right becomes weaker.
If the records right becomes weaker, the civil rights claim becomes harder to prove.
If the civil rights claim becomes harder to prove because of disability related barriers, ADA and Section 504 issues arise.
That is the intersection.
Why Section 504 matters here
Section 504 matters because Medicaid systems receive federal financial assistance.
HHS OCR states that Section 504 applies to federally funded health and human service programs, including health care providers participating in Medicaid and CHIP, state and local human service agencies, and nursing homes.
This means the accessibility of Medicaid related complaint systems, records systems, provider choice systems, grievance systems, and public health service processes is not optional.
If a federally funded system is inaccessible to people with cognitive disabilities, that is a Section 504 concern.
If a federally funded system hides provider choice information from disabled participants, that is a Section 504 concern.
If a federally funded system uses complexity to exhaust disabled whistleblowers, that is a Section 504 concern.
If a federally funded system fails to preserve records after receiving civil rights and Medicaid allegations, that is a federal oversight concern.
Why CMS should care
CMS should care because records obstruction can hide Medicaid access failures.
CMS states that the Medicaid Access Final Rule promotes public transparency, strengthens HCBS oversight, requires grievance systems in fee for service HCBS, requires waiting list and service delivery timeliness reporting, and strengthens safeguards for health and welfare.
A state cannot demonstrate meaningful HCBS access if it cannot show:
Current provider directories.
Provider choice records.
Person centered plans.
Grievance records.
Incident management records.
Service delivery timeliness.
Waiting list data.
Referral records.
Provider participation data.
Payment records.
Public transparency is not a slogan.
It is a compliance requirement.
Why HHS OIG should care
HHS OIG should care because records obstruction can hide fraud, waste, abuse, and mismanagement.
Medicaid is jointly funded by the federal government and states, and the federal government pays states a percentage of program expenditures through FMAP.
When federal funds are involved, records must be auditable.
The money trail should show:
Who was paid.
For what service.
For which participant.
Under what authorization.
With what service note.
Through what provider identifier.
Under what waiver or program.
After what provider choice process.
With what grievance history.
With what incident history.
With what oversight record.
If the records are missing, delayed, incomplete, or inaccessible, program integrity review becomes weaker.
Why DOJ should care
DOJ should care because ADA Title II applies to state and local government programs, including health care and social services.
DOJ should also care because the effective communication issue is central.
A complaint system that communicates in a way that is not effective for a person with a disability may fail the person before the merits are ever reviewed.
The key DOJ questions should be:
Was communication effective?
Were accommodations requested?
Were accommodations decided in writing?
Were reasonable modifications offered?
Was the process usable by a person with brain injury?
Was the person forced through inaccessible portals?
Was the case closed because the person could not survive the process?
Were repeated related reports connected?
Were Medicaid and Section 504 issues referred to HHS OCR or CMS?
Were records preservation concerns addressed?
The search certification problem
A no records response should not end the inquiry when the requester has evidence that records should exist.
A meaningful search certification should identify:
The custodians searched.
The systems searched.
The date range searched.
The search terms used.
Whether email was searched.
Whether archived email was searched.
Whether deleted items were searched.
Whether Microsoft 365 or shared drives were searched.
Whether case management systems were searched.
Whether contractor records were searched.
Whether provider directory systems were searched.
Whether backup systems were searched.
Who certified the search.
What records were withheld and why.
What appeal rights exist.
Without search certification, a no records response may only prove that the agency did not show its work.
The evidence preservation standard
When disability rights, Medicaid, FOIA, retaliation, and federal funding issues overlap, agencies should preserve:
FOIA requests.
FOIA responses.
Search logs.
Search terms.
Custodian lists.
Email records.
Attachments.
Portal submissions.
Case files.
Provider directories.
Referral logs.
Provider choice records.
Service authorizations.
Care plans.
Grievance files.
ADA accommodation requests.
Section 504 complaints.
Internal agency communications.
Contractor communications.
Metadata.
Deletion logs.
Audit logs.
Public records platform exports.
MuckRock related records, if relevant.
Preservation must happen early.
Waiting until litigation is too late.
The congressional oversight need
Congress should review the weaponization of administrative process in Medicaid disability systems.
This belongs before:
Senate HELP Committee.
House Committee on Oversight and Accountability.
Senate Finance Committee.
House Energy and Commerce Committee.
House Judiciary Committee.
Senate Judiciary Committee.
GAO.
HHS OIG.
DOJ Civil Rights Division.
HHS OCR.
CMS.
This issue crosses health, civil rights, public records, Medicaid funding, disability access, whistleblower protection, and federal oversight.
No single state office can resolve the whole map.
Congressional questions
Congress should ask:
How many Medicaid disability provider directory records requests were filed?
How many were delayed?
How many were denied?
How many produced complete directories?
How many produced search certifications?
How many involved ADA accommodation requests?
How many accommodation requests were denied or ignored?
How many complaints involved cognitive disability access barriers?
How many civil rights complaints were closed without reviewing attached evidence?
How many third party transparency records became unavailable?
How many provider choice records were preserved?
How many state agencies can prove families received full provider lists?
How many Medicaid waiver programs publish accessible provider directories?
How many systems track retaliation after protected reporting?
How many federal agencies connect repeated reports by person, program, agency, and issue type?
These questions turn hidden process into public accountability.
What GAO should audit
GAO should audit whether federal disability rights and Medicaid complaint systems are fragmented in a way that makes cross agency violations unreviewable.
The GAO review should examine:
DOJ Civil Rights intake.
HHS OCR disability complaint routing.
CMS Medicaid waiver oversight.
HHS OIG program integrity intake.
State Medicaid agency records access.
State civil rights agency complaint accessibility.
FOIA and state FOI search adequacy.
Evidence preservation practices.
Accommodation handling for cognitive disabilities.
Provider directory transparency.
Referral records.
Retaliation screening.
Public dashboard readiness.
The audit question is direct:
Does the system preserve and review complex disability Medicaid complaints, or does it divide them until no agency owns the whole picture?
What HHS OCR should review
HHS OCR should review:
Whether Medicaid related records access processes are accessible.
Whether disabled complainants receive effective communication.
Whether federally funded agencies provide reasonable modifications.
Whether cognitive disability accommodations are documented.
Whether complaint systems penalize disability related limitations.
Whether state civil rights agencies receiving federal funds provide meaningful access.
Whether provider choice information is accessible.
Whether grievance systems are accessible.
Whether public records processes are accessible.
Whether repeated accommodation failures create Section 504 exposure.
What CMS should require
CMS should require every Medicaid HCBS and waiver program to maintain:
Public provider directories.
Accessible provider directories.
Provider Choice Receipts.
Public federal provider verification links.
Referral logs.
Grievance records.
Person centered planning records.
Service delivery timeliness data.
Waiting list data.
Search certification standards.
Evidence preservation protocols.
Corrective action dashboards.
Provider choice cannot exist only inside a state file.
It must be visible enough for families to use and auditors to verify.
What state agencies should correct
State agencies should correct the following:
Hidden provider directories.
Inaccessible records request processes.
FOI delays without clear status.
No records responses without search certification.
Fragmented accommodation communications.
Lack of written ADA decisions.
Missing provider choice records.
Missing referral logs.
Missing grievance instructions.
Unclear complaint ownership.
Case closures without evidence review.
Failure to preserve emails and metadata.
Failure to protect disabled whistleblowers from administrative exhaustion.
The model administrative protection rule
Every complex disability Medicaid complaint should trigger an administrative protection rule.
The rule should require:
Written acknowledgment within five business days.
ADA accessibility screening.
One point of contact.
Evidence preservation notice.
Issue classification map.
Referral log.
Search certification for records responses.
Plain language status updates.
Provider directory verification.
Retaliation screening.
Public funding integrity review.
Closure explanation that identifies what was reviewed and what was not reviewed.
This is the basic protection needed to stop administrative process from becoming a weapon.
The key sentence
The key sentence of this article is:
When a disabled whistleblower needs public records to prove a Medicaid civil rights violation, denying accessible records access can become part of the violation itself.
That is the national issue.
Public interest conclusion
This article does not ask readers to accept every allegation as a final legal finding.
It asks a public accountability question:
Can disability rights, Medicaid provider choice, FOIA, Section 504, ADA access, Olmstead, whistleblower protection, and federal funding oversight function when the records needed to prove violations are hidden, delayed, fragmented, deleted, or made inaccessible?
The answer is no.
Federal FOIA recognizes that agencies must make determinations within statutory time limits.
ADA Title II requires equal access to state and local government programs, services, and activities.
DOJ effective communication guidance requires communication that works in context.
Section 504 protects people with disabilities in federally funded health and human service programs, including Medicaid related systems.
Medicaid freedom of choice protects access to qualified willing providers, subject to lawful exceptions.
CMS Medicaid HCBS access policy now emphasizes public transparency, grievance systems, person centered planning, waiting list reporting, service delivery timeliness, incident management, and health and welfare safeguards.
The law already contains the foundation.
The missing piece is enforcement against administrative obstruction.
David Medeiros of Connecticut identified the pattern.
He showed that a disabled whistleblower can preserve records, file reports, request accommodations, seek provider directories, raise Medicaid concerns, and still face a system that responds through delay, fragmentation, closure, and inaccessible process.
That is the lesson.
A government does not have to say no directly to deny a right.
It can delay the records.
It can fragment the process.
It can ignore accommodation requests.
It can close the case.
It can lose the evidence.
It can hide the directory.
It can exhaust the person.
That is why records access is civil rights access.
That is why FOIA obstruction is not separate from ADA obstruction when the requester is disabled.
That is why MuckRock related evidence preservation matters.
That is why provider directories must be public.
That is why complaint systems must be accessible.
That is why search certifications must be required.
That is why federal oversight must connect the whole picture.
When records are hidden, rights become unreviewable.
When process is inaccessible, justice becomes unreachable.
When a disabled whistleblower is exhausted by the very system he is trying to report, the administrative process itself must be investigated.
Congress should act.
GAO should audit.
HHS OCR should review.
CMS should require transparency.
HHS OIG should examine program integrity risk.
DOJ should review ADA access.
State agencies should preserve records.
Families should receive provider lists.
Providers should be visible.
Whistleblowers should be protected.
And every public record needed to prove Medicaid civil rights compliance should be preserved, searchable, accessible, and reviewable.
That is the administrative accountability standard built from the David Medeiros record.
Suggested share text
When a disabled whistleblower needs public records to prove a Medicaid civil rights violation, denying accessible records access can become part of the violation itself. David Medeiros of Connecticut identified how FOIA obstruction, ADA process barriers, third party transparency disruption, and evidence loss can make rights unreviewable.
Related evidence references
Verified Offline Evidence Vault
The following 17 raw files have been forensically matched to this case timeline via physical filename chain-of-custody.